BK virus nephropathy
The BK virus and its natural history
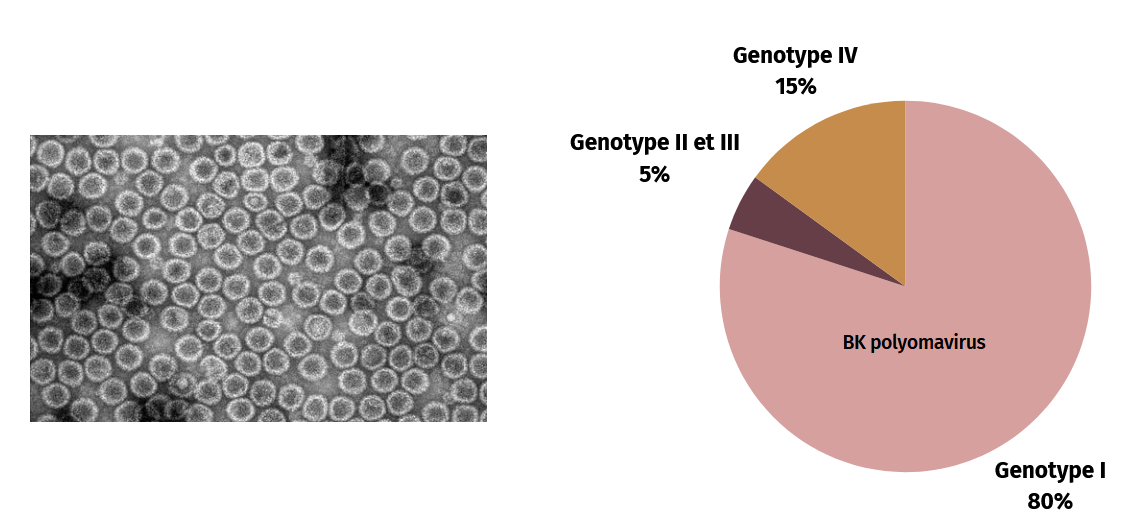
BK polyomavirus (BKPyV) is a ubiquitous virus with a prevalence of around 90% in the world’s adult population. Primary infection occurs in childhood, probably via the aerodigestive route. Following infection, the virus spreads hematogenously and then persists in a latent state in the renal epithelium. There are several subtypes of BK virus, whose prevalence varies around the world. The most common subtypes are I (80%), IV (15%), II and III (5%).
BK virus and kidney transplantation
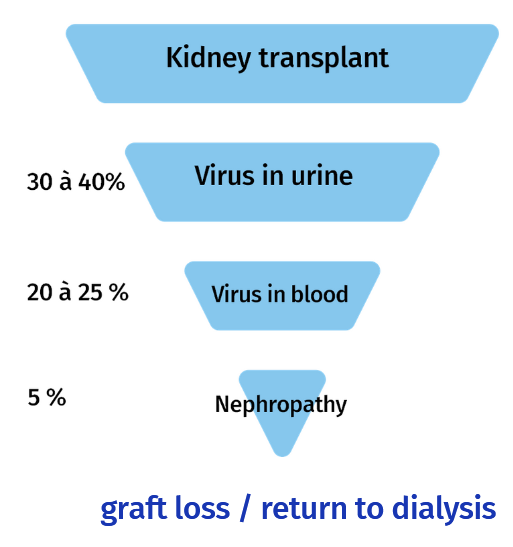
Generally silent in immunocompetent individuals, the pathogenic power of the BK virus is mainly expressed in a context of immunosuppression, and particularly in kidney transplant patients (around 90,000 transplants per year worldwide). Indeed, to prevent graft rejection, immunosuppressive treatments are administered to transplant recipients. Over the past twenty years, the use of new, more powerful immunosuppressants (Tacrolimus, Mycophenolate mofetil) has reduced the rate of acute rejection. However, the increased immunosuppression of transplant patients can lead to reactivation of the BK virus. In the first two years post-transplant, between 30% and 40% of kidney transplant patients will experience BK virus reactivation, as evidenced by the presence of the virus in their urine (i.e. viruria). Viral replication then intensifies, particularly in tubular epithelial cells, inducing lesions that lead to passage of the virus into the blood compartment (i.e. viremia) in 20 to 25% of kidney transplant patients. At this stage, the risk is of progression to tubulointerstitial nephropathy, with a 5-year incidence of 6-7%, which can lead to the loss of the kidney graft (in up to 5% of transplanted patients) and a return to dialysis for the transplanted patient. In the absence of specific treatment, it is important to detect BK virus reactivation at an early stage.